
The Thrower’s Shoulder (Part 1): The Functional and Relevant Anatomy of the Shoulder Complex
The shoulder is the most mobile joint in the human body with a remarkable range of motion. The shoulder has an ability to move within 3 degrees of freedom (DOF): Flexion & Extension, Abduction & Adduction, Internal Rotation & External Rotation. The mobility of the shoulder allows it to complete an incredibly versatile range of movements and produce large amounts of rotational motion. However, this mobility can come at the cost of joint stability. The shoulder, especially in throwers, is susceptible to instability, laxity, and inert tissue tears more so than most others in the body.
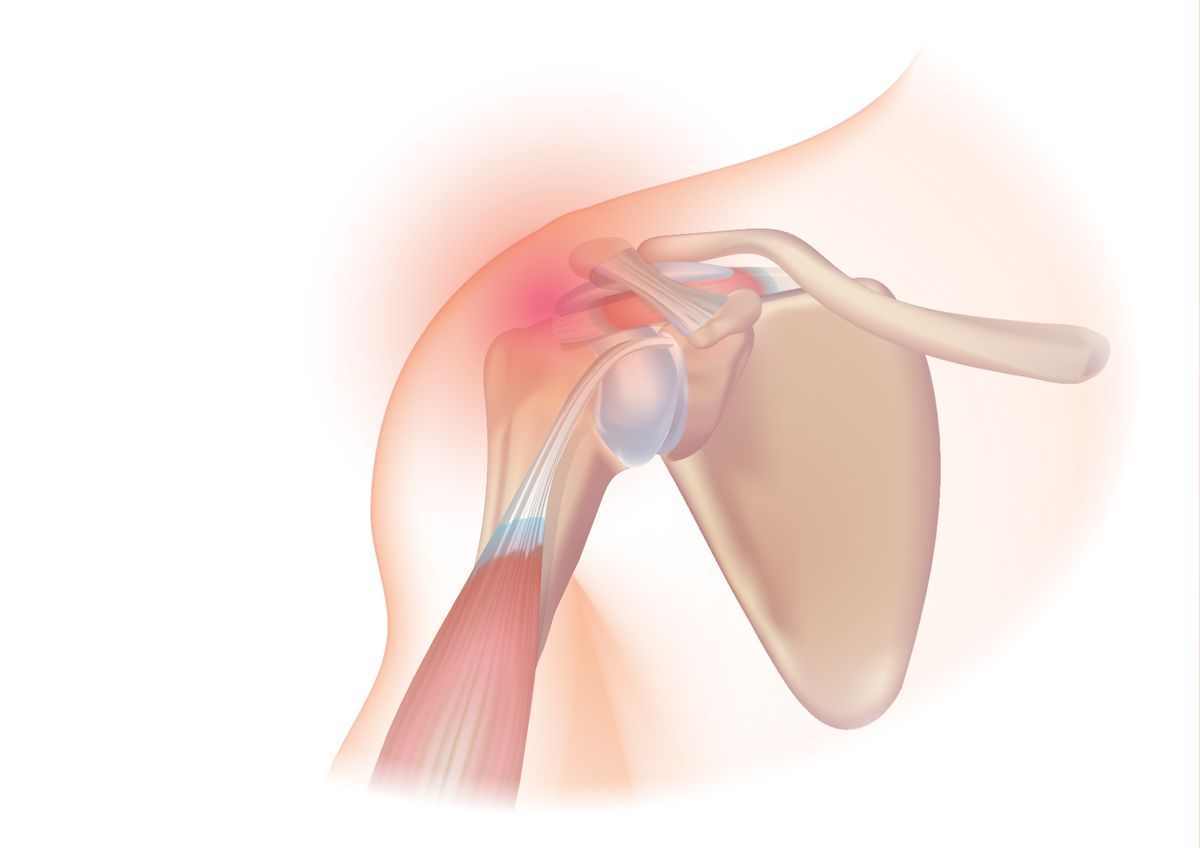
In order to best understand the biomechanics of the shoulder in Part 2 and the complete applied biomechanics to throwing in Part 3, we first need to examine the relevant anatomy, both structure and function, of the glenohumeral joint complex (shoulder). Additionally, it is important to introduce the concept of joint arthrokinematics and why they play a large role in the shoulder’s performance, but also its inherent injury risk in throwers. Although all structures play an important role in the function of the shoulder, some anatomical areas are “more important” when it comes to the functional process of throwing as it relates to the shoulder anatomy. Below I will list all functional shoulder anatomy, but also highlight (bold) the areas which will be most notable.
If you're interested in QB specific throwing, lifting and sprint training, customized to you, with the same systems used to train NFL Quarterbacks, take the assessment and get the app at kinetex.co. If you're interested in reading about all things quarterbacking and throwing biomechanics, subscribe to the blog.
Anatomy:
Bone:
- Clavicle (Collarbone)
- Scapula (Shoulder Blade)
- Acromion Process
- Coracoid Process
- Scapular Spine
- Glenoid Cavity
- Humerus (Upper Arm)
Muscles:
- Rotator Cuff
- Supraspinatus
- “Posterior Cuff”
- Infraspinatus
- Teres Minor
- Subscapularis (Subscap)
- Biceps Brachii
- Long head of Biceps
- Short head of Biceps
- Triceps
- Long head of Triceps
- Lateral head of Triceps
- Medial (Short) head of Triceps
- Pectoralis Major (Pec Major)
- Pectoralis Minor (Pec Minor)
- Teres Major
- Latissimus Dorsi (Lat)
- Deltoid
- Anterior Deltoid (Front Delt)
- Lateral Deltoid (Side Delt)
- Posterior Deltoid (Rear Delt)
- Upper Trapezius (Upper Trap)
- Lower Trapezius (Lower Trap)
- Serratus Anterior (Serratus)
- Rhomboids
- Levator Scapulae
Ligaments:
- Glenohumeral Ligaments
- Superior (SGHL)
- Middle (MGHL)
- Inferior (IGHL)
- Coracohumeral Ligament
- Acromioclavicular Ligament (AC)
- Coracoclavicular Ligament (CC)
- Conoid Ligament
- Trapezoid Ligament
- Transverse Humeral Ligament
- Ligamentum Teres
Labrum
- Superior Labrum
- Anterior Labrum
- Posterior Labrum
Nerves and Vessels:
- Brachial Plexus
- Subclavian Artery & Vein
- Axillary Artery & Vein
Joints:
- Glenohumeral Joint (GHJ)
- Acromioclavicular Joint (ACJ)
- Sternoclavicular (SCJ)
Capsule
- Bursae
Here is a link where you can click around to visualize each part of the anatomy listed above and below.
Main Points for Important Anatomy
Scapula: Attachment site for the rotator cuff origins. The motions of the scapula play an important role in allowing full range of motion of the shoulder. If scapular movement is limited there can be a reduction in mobility and or a propensity to impact the rotator cuff tendons (impingement, tearing).
Acromion Process: The acromion is a part of the scapula and lies on top of the “Subacromial Space” which is where the rotator cuff tendons pass under. The acromion process can have bony changes occur through life making the likelihood of impingement or tearing of the rotator interval more likely. Notably, poor posturing, rounded shoulders, or a tight pec minor can cause tipping or tilting of the scapula, pushing the acromion process closer to the subacromial space and impacting the rotator cuff tendons over time.
Glenoid Fossa: Glenoid fossa is a part of the actual scapula and is the point of contact for the humeral head (arm bone). The fossa is a shallow, concave, oval aspect of the glenoid. It is considered a shallow “socket” for the shoulder to create a joint with. The anatomy of the glenoid fossa is central to the function and movements of the shoulder, making it a critical part of the shoulder’s complex structure and enhanced mobility.
Humerus: Upper arm bone which is the attachment point for the rotator cuff, lats, biceps, triceps, deltoid, etc. In throwers the humerus can grow into more external rotation bias “retroversion” if an athlete performed high intensity throwing during puberty. This can be a productive response for total rotational arc and velocity but also requires special testing measures to properly measure the arm.
Supraspinatus: Produces abduction (lifting arm to the side) of the arm from rest to 15-30 degrees. Helps provide a force couple against deltoid to best provide smooth motion of overhead activity. Additionally, as with all rotator cuff muscles, co-contractions serve to provide stability and ensure smooth, controlled movement of the arm.
Infraspinatus: The primary function of the infraspinatus muscle is to externally rotate the arm. It is the most active external rotator when the arm is 90 degrees of abduction (high five position or throwing position). This is the main function activated both concentrically and eccentrically when throwing a ball. Additionally, as with all rotator cuff muscles, co-contractions serve to provide stability and ensure smooth controlled movement of the arm.
Teres Minor: The primary function of the teres minor is to externally rotate the arm. The teres minor is more active when the arm is positioned at the side of the body and during movements that involve external rotation. It works closely with the infraspinatus to achieve external rotation.
Subscapularis: The primary function of the subscapularis is to internally rotate the arm. Internal rotation of the arm happens during the acceleration and release phase of the arm. In addition to its role in internal rotation, the subscapularis muscle also helps to stabilize the humeral head with compression to the glenoid.
Long Head of Biceps: Long head of the biceps inserts at the superior labrum and supraglenoid tubercle. The long head of biceps assists with shoulder flexion. Most importantly in throwing, the long head of the biceps plays a role in deceleration of the arm during the release of throwing. Along with the rotator cuff muscles the long head of the biceps helps to provide dynamic stability to the shoulder. Due to the attachment of the LHBT to the labrum, there is a propensity for a “peel-back” mechanism of the bicep on the labrum during throwing causing a “SLAP” tear. SLAP tears will be explained in Part 2.
Pectoralis Minor: The pec minor inserts on the coracoid process of the scapula. It works to create downward rotation of the scapula, and increased tension or stiffness in the pec minor prevents normal and fluid upward rotation needed for overhead activities such as throwing.
Latissimus Dorsi: The lat attaches to the humerus and creates arm adduction (moving closer to the body), arm extension, and aids in arm internal rotation. It is one of the most powerful muscles in the body and spans a large surface area with attachments to the arm, scapula (in up to 80% of the population), lumbar spine (thoracolumbarfascia), thoracic vertebrae, lumbar vertebrae, top of the hip bone (iliac crest), and lower ribs. The lat plays an important role in arm deceleration, handling large amounts of eccentric stress. It can also contribute to or limit hip-shoulder separation angle and rotational mobility of the spine.
Capsule: The shoulder capsule is a fibrous structure surrounding the shoulder. It includes the ligaments, synovial membrane, and other inert tissues that enclose the joint, providing stability and protection. The shoulder capsule helps keep the head of the humerus properly seated within the shallow glenoid cavity of the scapula along with the suction of the labrum. This is crucial for maintaining joint integrity and allowing a wide range of motion. The capsule has a propensity to stretch out anteriorly (in the front) with repetitive high stress throwing creating instability.
Inferior Glenohumeral Ligament: The inferior glenohumeral ligament (IGHL) plays a role in limiting posterior movement during throwing. It becomes taut during abduction and external rotation of the shoulder. The posterior band of the IGHL helps stabilize the joint and prevents excessive posterior translation of the humeral head. This is important in protecting the shoulder joint during the dynamic and high-velocity movements involved in throwing.
Acromioclavicular Joint: The joint at the top outside part of the shoulder where the clavicle (collarbone) and acromion meet.
Acromioclavicular Ligament: Supports and stabilizes the junction where the clavicle and acromion meet.
Coracoclavicular Ligament: Supports and stabilizes the clavicle in a downward fashion. The anchoring effect of this ligament gives the clavicle stability needed for its smooth and secure movement in conjunction with the scapula.
Superior Labrum: The top part of the labrum where the bicep tendon also inserts. Often injured in throwers with a “SLAP” tear (Superior Labrum Anterior to Posterior).
Subclavian, Axillary, or Brachial Artery: The vascular structures that can be compressed between the clavicle and first rib space either due to first rib elevation, posturing, or tight musculature. This compression of these vessels or nerves in the shoulder is called Thoracic Outlet Syndrome or TOS and is most common in high intensity throwers. TOS can vary in severity and presentation. Arterial vascular compression is more common in the neurogenic type of TOS, which involves compression of the brachial plexus.
Upper Trap, Lower Trap, Serratus Anterior Muscles: Three muscles that work together in a fluid and coupled motion that provides the forces necessary to move the scapula upward lay and create the required rhythm, range and space for the humerus (arm) to move freely overhead and into rotation. The Serratus plays an especially important role in throwers due to the dominance of the trap and (usually) relatively untrained nature of the Serratus causing an imbalance in the force-couple.
Part 2 will discuss how these specific pieces of anatomy play an important role in the biomechanics of the shoulder, especially in relation to throwing. Additionally, I will discuss how they can enhance performance but also cascade in potential increased injury risk.
If you're interested in QB specific throwing, lifting and sprint training, customized to you, with the same systems used to train NFL Quarterbacks, take the assessment and get the app at kinetex.co. If you're interested in reading about all things quarterbacking and throwing biomechanics, subscribe to the blog.